
Why the Creatine You Take Barely Reaches Your Brain
The honest science behind why oral creatine only raises brain levels by 5 to 15 percent, what is actually limiting it, and what researchers are building to solve the problem.


The last article established one clear answer for muscle creatine: plain monohydrate, taken consistently, is what thirty years of research supports. That answer holds. But if your reason for taking creatine goes beyond muscle performance — if you are interested in what it does for your brain — the story changes. The same supplement. A different biological problem. And a ceiling that no amount of standard monohydrate overcomes.
The Transporter Bottleneck
The blood-brain barrier controls what gets into the brain and what does not. Creatine does not get a free pass. It can only cross through a specific molecular gateway called SLC6A8, a transporter protein that sits in the walls of the tiny blood vessels feeding the brain. Without it, creatine cannot get in.
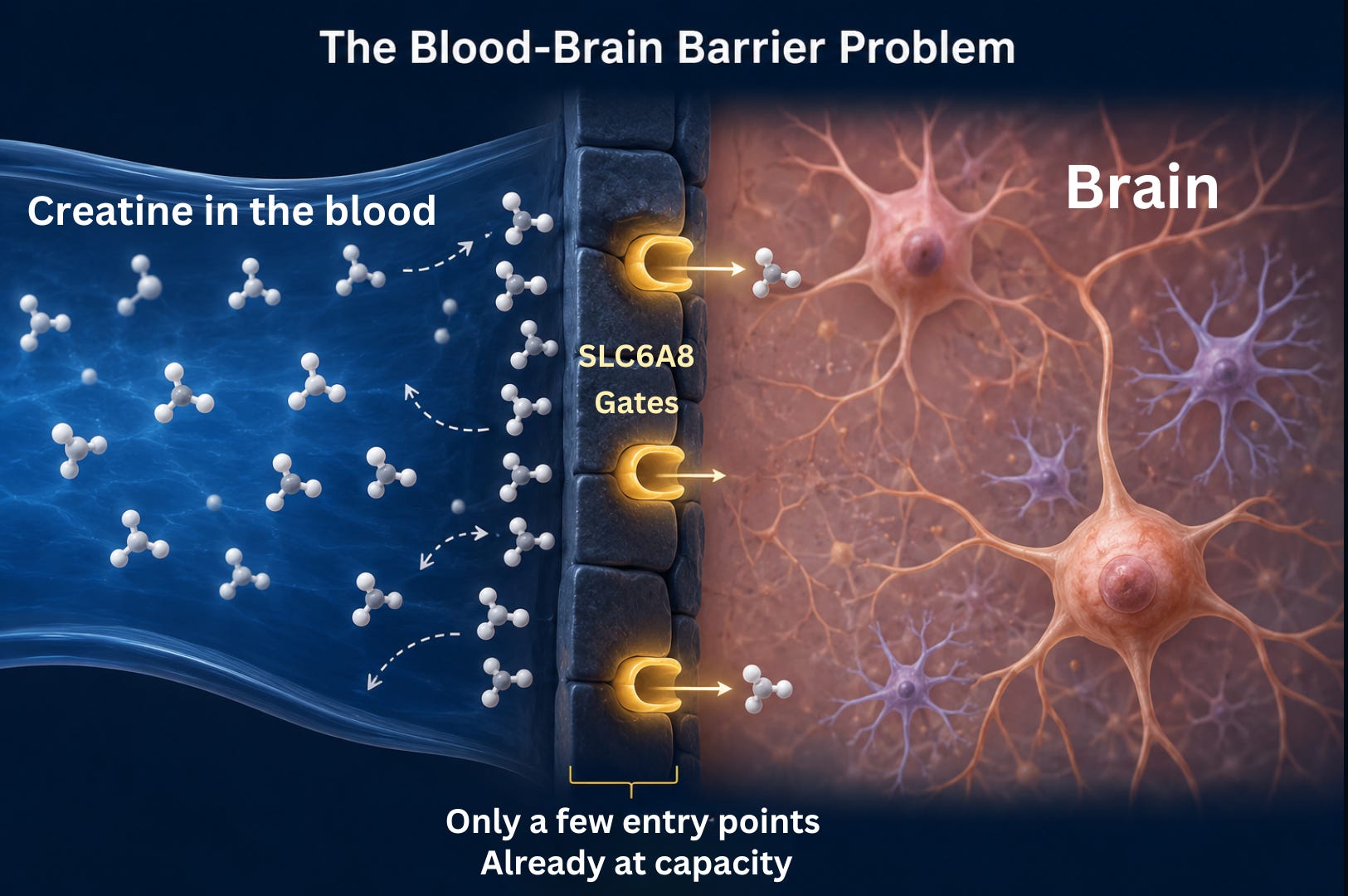
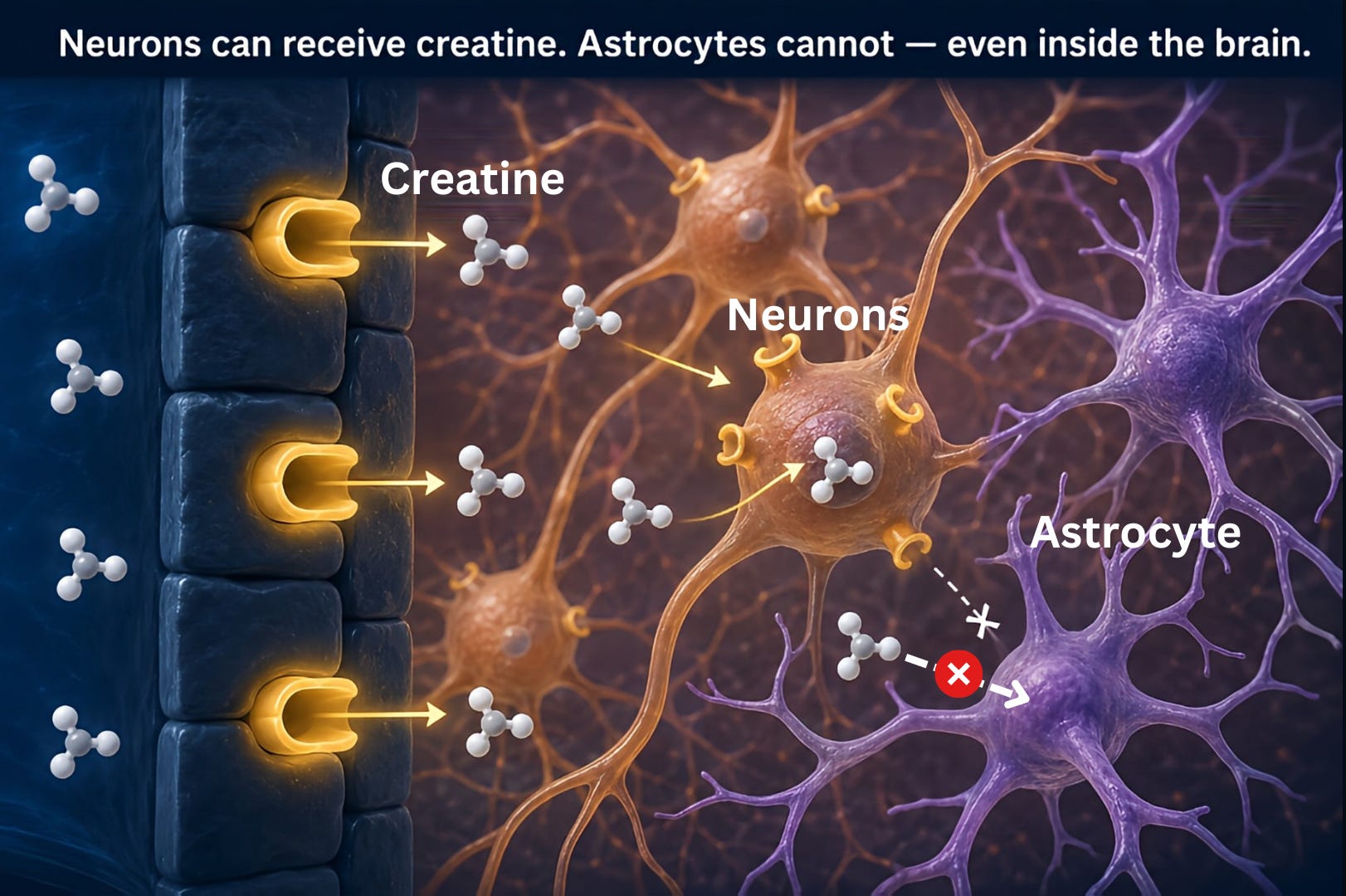
This gateway is rare. It is present in the blood vessel walls and in neurons, but it is missing from astrocytes, the cells that make up much of the brain’s volume. Astrocytes can produce some creatine locally through their own synthesis machinery, but they cannot absorb it from the bloodstream. So Creatine from food or supplements has to find one of those specific entry points and wait its turn.
The gateway also has a maximum capacity. Standard oral supplementation already pushes it to or near its limit. Taking more creatine does not open more gates. There is also evidence that chronic high dosing can cause the brain to reduce the number of available transporters over time as a compensatory response — meaning very high long-term doses may work against themselves. Think of a busy train station with only one working ticket barrier. Doubling the crowd outside does not speed things up. The barrier is already processing as fast as it can.
This is why researchers are no longer asking how much creatine to take for the brain. They are asking how to get around the gateway entirely. That is what the approaches covered later in this article are trying to solve. The ceiling is not a dosing problem. It is structural.
What Oral Supplementation Actually Achieves in the Brain
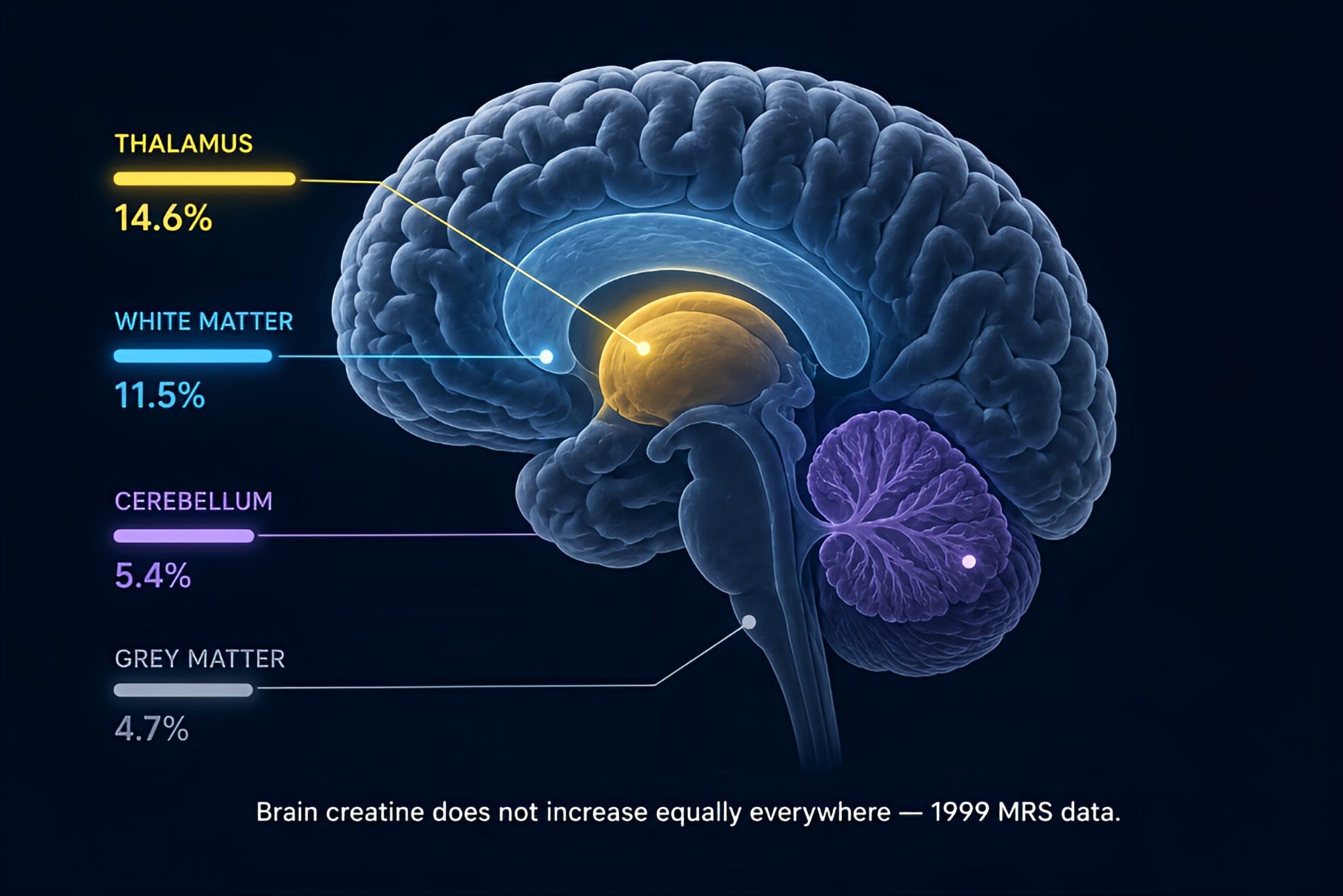
Dechent and colleagues measured brain creatine directly using magnetic resonance spectroscopy in 1999. They gave 20 grams per day — split into four 5-gram doses — for four weeks, resulting in a statistically significant 8.7 percent increase in total brain creatine averaged across regions in healthy young volunteers. The increase was not uniform: the thalamus showed the largest rise at 14.6 percent, white matter at 11.5 percent, cerebellum at 5.4 percent, and grey matter at 4.7 percent.
Other MRS studies using higher doses have reported increases in brain creatine ranging from 5 to 15%. Getting there takes time. Even the lower end of that range typically needs at least four weeks of consistent supplementation. Muscle creatine saturates within one to two weeks at standard doses. The brain is slower and less complete by comparison.
That 5 to 15 percent increase is real and does appear to influence outcomes in some contexts. But understanding what creatine actually does in the brain changes how you interpret those numbers.
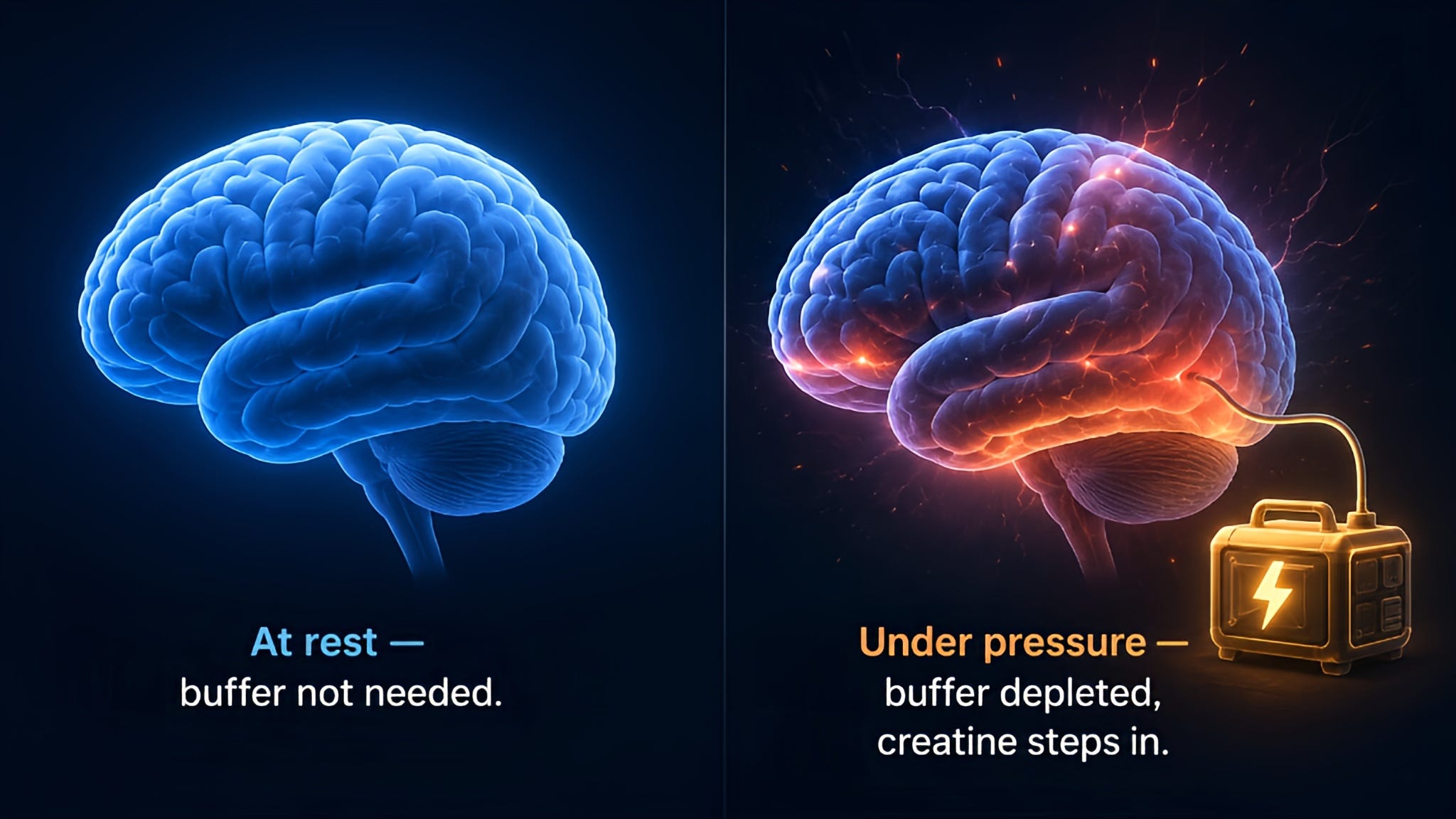
Creatine does not fuel the brain at rest. It acts as an energy buffer — a reserve that gets drawn on when the brain’s demand for ATP spikes suddenly and the normal supply cannot keep up fast enough. Think of it less like adding fuel to a tank and more like adding a backup generator. At rest, when the main power supply is adequate, the generator sits idle. Under stress, sleep deprivation, or intense cognitive load, the generator becomes the difference between the lights staying on and flickering.
Creatine does not make a well-rested brain sharper. What it does is rescue performance when the brain is under pressure — during sleep deprivation, mental fatigue, or intense cognitive demand. That is when the backup generator matters. It also helps explain why cognitive trials show inconsistent results: a study measuring prefrontal function in sleep-deprived participants will find a different answer than one measuring memory in well-rested young adults, even at the same dose.
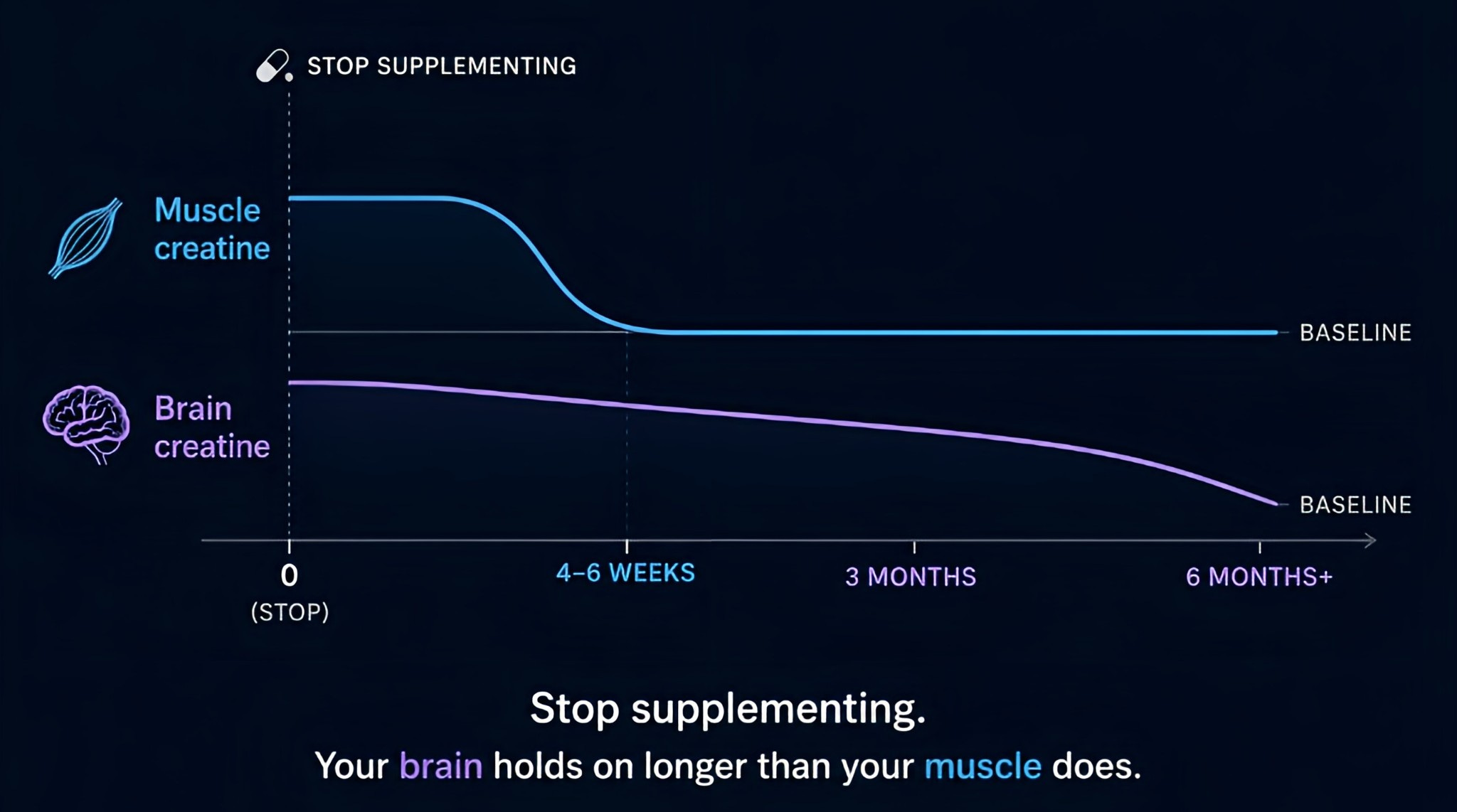
One practical implication worth noting is that a short gap in creatine dosing matters less for brain function than for muscle performance. Once brain creatine levels rise, they remain elevated for weeks to months after stopping supplementation, significantly longer than muscle creatine, which drops back to baseline within 4 to 6 weeks.
Regional Brain Differences
Brain creatine does not increase equally across all regions after supplementation. The regions that respond most are those with the highest baseline energy demand — the frontal cortex and thalamus draw heavily on the creatine buffer during normal function and show the greatest increases when that buffer is expanded. The hippocampus and grey matter respond less. This is consistent with what the Dechent data showed: thalamus at 14.6 percent, white matter at 11.5 percent, cerebellum at 5.4 percent, grey matter at 4.7 percent.
Part of why this pattern went unrecognized for so long is a technical one. Early MRS studies used low-resolution methods that could not map regional differences with sufficient precision. The literature looked more consistent than it actually was because the tools were not sensitive enough to show the variation.
This regional pattern almost certainly explains some of the inconsistency across cognitive trials in Parkinson’s and Alzheimer’s. A trial measuring working memory in a task that relies heavily on prefrontal function may see a meaningful benefit. A trial measuring hippocampal-dependent episodic memory at the same dose may see nothing. The dose, the duration, and the population are identical. The brain region driving the outcome is not.
The CONCRET-MENOPA frontal brain creatine finding directly fits this pattern. The frontal cortex appears to be among the more responsive regions, which is consistent with the executive function and reaction time improvements that the trial measured.
Why This Gap Matters
The cognitive research on creatine has used doses of 3 to 8 grams per day. The brain creatine increases at those doses are 5 to 15%, not the near-complete saturation achievable in muscle. The BBB transporter becomes saturated before the brain reaches that point. This is the structural reason why pharmaceutical companies keep inventing new compounds: the ceiling on oral delivery is real, and getting around it requires either a different molecule or a different delivery route.
The Bottom Line
Oral creatine monohydrate is not ineffective for the brain. It meaningfully raises brain creatine, and that increase matters under the right conditions. But the ceiling is structural, not a dosing failure. And the brain’s own production system, while remarkable, cannot fully close the gap on its own.
The question this article raises — how do you actually get more creatine into the brain, and what happens when you do — is what the next article answers.
This is just the beginning of the Creatine Brain Series.
We have already covered:
What Creatine Actually Does to Your Brain — Importance of creatine to your brain health
Creatine for the Healthy Brain: Dose, Timing and Real Effects — The specific protocols to supplement creatine, and who could be deficient and what you should do
Your Steak Is Lying to You: The Creatine Content Reality — How much creatine do you get from cooked food
Your Creatine Baseline Exists. Medicine Just Cannot Measure It Yet — Methods to measure your creatine baseline
Not All Creatine Is the Same — The honest science-based breakdown of every creatine form on the market
What I will talk about as we go through this series into a booklet is:
Why the cheapest supplement barely reaches your brain — and the emerging compounds that might actually fix that
GAA: the creatine precursor that crosses the blood-brain barrier differently
Who responds most to brain-targeted creatine — and why your biology determines the answer
Creatine in disease, recovery, aging, and high-performance states
Fascinating post. I was taking 5 grams daily creatine for six+ months—partly for muscles, partly for brain. Elevated creatine levels were detected in my annual bloodwork, so I stopped. Getting another blood test soon to see if levels have normalized, then I guess I’ll go from there. Look forward to reading more of this series!
Interesting overview, but it assumes that getting more creatine into the brain is automatically better without asking whether we have actually studied the long term consequences. Most creatine safety studies rely on routine blood work and adverse event reporting, not detailed assessments of mitochondrial function, neuroenergetics, brain imaging, or metabolic flexibility. Before we start trying to bypass the brain's own transport controls, it seems reasonable to ask whether those controls exist for a reason.