
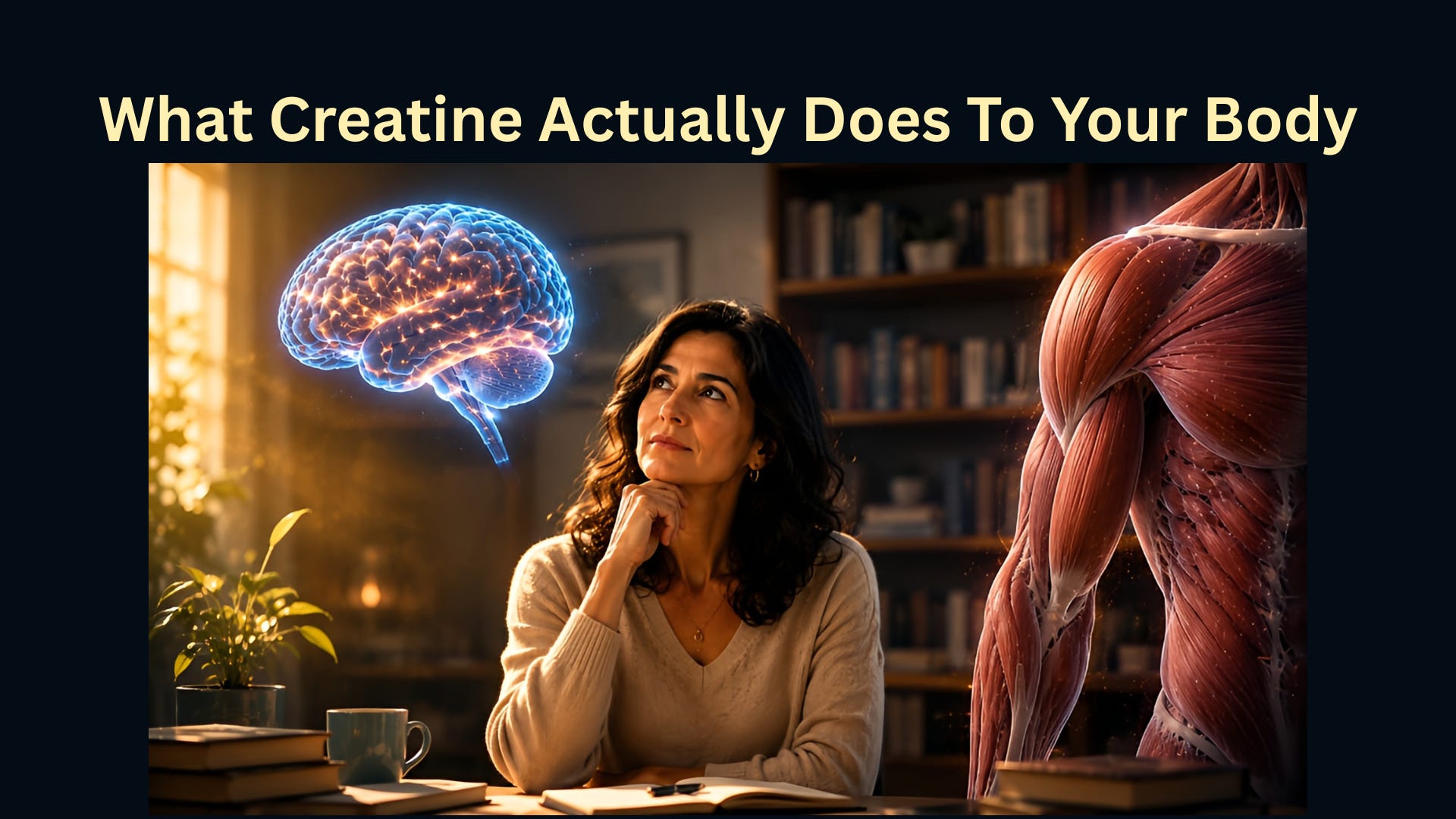
What Creatine Actually Does To Your Body
It is not what the bodybuilding world told you — and it is more interesting.

Nadia is 47. She teaches high school. She is not an athlete, not sick, not deep in the wellness world.
But three things happened in the same month. Her gym colleague, also in her mid-40s and not an athlete, started taking creatine and kept saying her energy was better. Then Nadia heard it mentioned on a longevity podcast. Not a fitness podcast — a longevity one, the kind that talks about mitochondrial function and inflammation markers. And then she came across it being discussed in a thread about brain fog in perimenopause.
She Googled it and got bodybuilding forums, supplement ads, and a Reddit argument about kidney damage. She sighed and closed all the tabs.
Nadia just wanted a simple answer: what does creatine actually do? Not what a salesperson claims, but what does biology say? Can it be beneficial to me?
This article aims to provide a clear, science-based explanation of what creatine does in your body, separating the biological facts from marketing and online claims, and clarifying whether there are benefits beyond bodybuilding.
Your body already makes creatine.
The first thing worth knowing, and it tends to surprise people, is that creatine is not foreign to your body. You are already making it. Every day, your liver, kidneys, and pancreas synthesize creatine from amino acids. You also get it from food: a standard serving of beef or salmon contains roughly one to two grams.
If you eat meat regularly, your body currently contains 120–140 grams of creatine, most of which is stored in skeletal muscle. By contrast, if you eat little or no meat, as in Nadia’s case, where she has chicken once or twice a week and rarely eats red meat, your body stores are typically 10–20% lower than average.
That gap in storage or having lower creatine levels is not a disease. But it matters once you understand what creatine actually does inside your cells.
The mechanism: phosphocreatine and the ATP problem
Your cells run on ATP (adenosine triphosphate), the molecule your body uses as energy currency. Every muscle contraction, every neuron firing, every single heartbeat spends ATP. The problem is that your cells cannot store much of it. At full exertion, you could exhaust your entire supply in seconds.
This is the problem creatine solves.
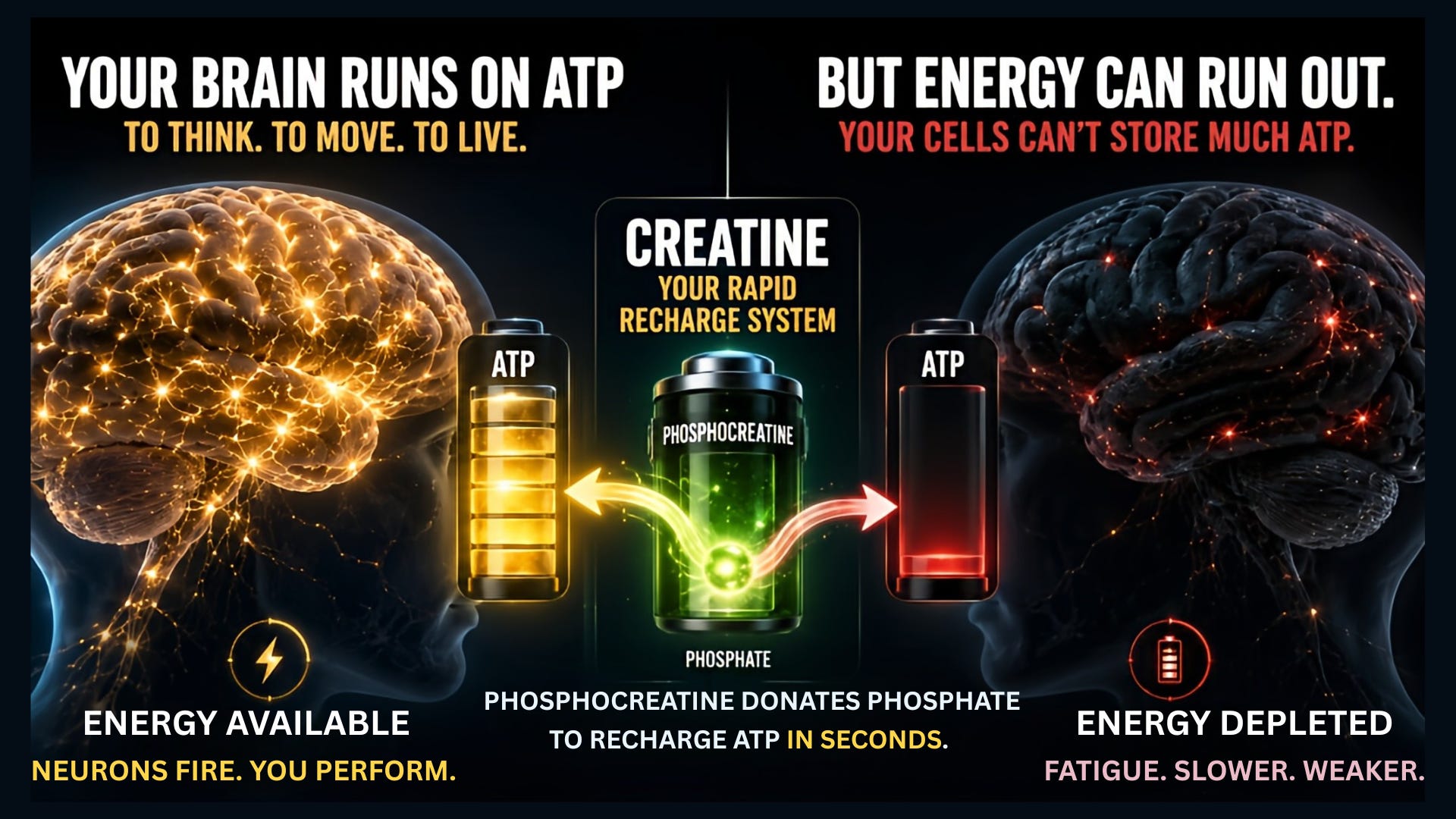
Inside your cells, creatine exists in two forms: free creatine and phosphocreatine. Phosphocreatine carries an extra phosphate group. When your ATP, the energy currency, runs low, phosphocreatine donates a phosphate group to regenerate it almost instantaneously. The reaction takes less than a second.
Here is a way to picture it: ATP is the fuel your cells actually burn. Phosphocreatine is the reserve tank that refills the fuel on demand, faster than any other system in your body.
This is why athletes first noticed creatine. Explosive efforts like sprinting and heavy lifting demand rapid ATP turnover, and this is exactly where the phosphocreatine system matters most. The performance data is among the most replicated findings in sports science.
Why your brain cares about this more than your muscles do
Here is where it gets more interesting than the bodybuilding world let on.
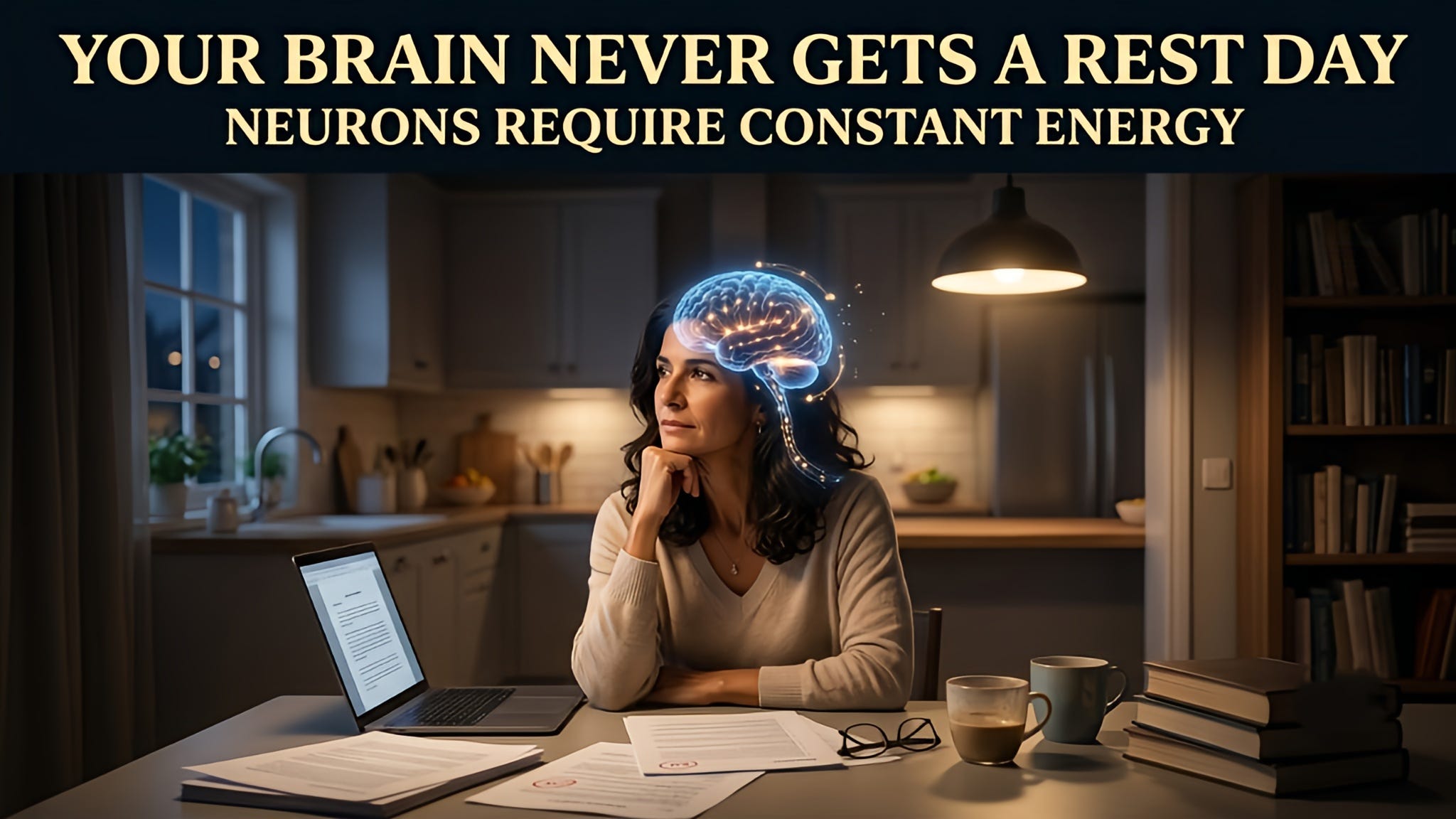
Your brain is about 2% of your body weight. It consumes about 20% of your body’s energy. Neurons fire constantly, processing, signaling, and regulating, and every single firing costs ATP. Unlike muscle, your brain does not get rest days.
Brain cells maintain their own creatine supply independently of the rest of the body. In practice, this means that when neurons are under metabolic stress, sufficient brain creatine availability can keep them firing continuously. Run that supply low and neuronal function suffers. This is established biology, not a hypothesis.
This is why researchers began investigating creatine and its links to cognition: not from a theoretical leap, but from the mechanism itself. The rationale follows directly from the mechanism. Neurons are among the highest energy users in the body, and they depend on the phosphocreatine system to keep firing under demand. If that rapid-recharge system matters anywhere, it matters in the brain.
Nadia’s question, whether creatine could help with the cognitive fatigue she has noticed this year, is scientifically reasonable. Whether the evidence supports it for someone in her situation is a different question. That is what the next article covers.
What happens at the extremes
The clearest evidence of how essential creatine is comes from rare cases in which the body cannot make or transport it at all, suggesting that a component of the creatine metabolic pathway is mutated or nonfunctional. When that happens, the consequences show up early. Genetic mutations that affect creatine synthesis or the cellular transport of creatine can result in serious childhood conditions such as intellectual disability, language delays, and seizures. I raise this not to alarm, but because nothing illustrates the stakes of a molecule more clearly than its complete absence or its lack of natural functionality in the body.
Most people reading this are nowhere near clinical deficiency. But there is a meaningful spectrum between clinical absence and optimal levels, and more people sit closer to the lower end than they might expect.
Vegetarians and vegans are the best example. Without dietary meat or fish, the body relies entirely on its own ability to synthesize and distribute creatine. Studies have consistently shown that vegetarians’ muscle and brain creatine levels are lower than those of omnivores.
Older adults are another. Creatine synthesis declines with age, quietly and without obvious outward symptoms at first. But a decline in creatine could lead to fatigue and cognitive slowing, and is usually blamed on “aging” rather than addressing creatine as a root cause.
Women in perimenopause and menopause are a group that researchers are only beginning to study properly in this context. Hormonal shifts broadly affect energy metabolism, and early data suggest that creatine levels may also be affected.
And then there is the category that does not get discussed enough: outwardly healthy people under sustained cognitive load, not athletes, not patients, just people whose minds do not get to clock out, whose days run long and whose sleep runs short, who may be drawing on their creatine reserves at a higher rate than they are replenishing them.


On the upper end, excess creatine is converted to creatinine and excreted in urine. This means your blood creatinine level will rise when you supplement. This is expected and does not indicate kidney damage, though the confusion between the two is one of the most common misunderstandings in this space, and one I will address directly in a later piece.
At high doses, some people experience gastrointestinal discomfort, bloating, and nausea. Splitting doses across the day typically resolves this issue. But high doses for several years can have their side effects too. We will talk more about this soon.
What the hype gets right, and where it overreaches
Creatine is one of the most studied supplements ever tested in clinical trials. The mechanism is well established, and the athletic performance data are solid across a wide range of populations, from competitive athletes to older adults. More recently, researchers have begun to ask what creatine does for the brain and long-term health. The early findings are interesting. The conclusions are not yet.
But the hype consistently overreaches in three directions.
Scope. Creatine is not a treatment for any disease. Some of the claims circulating online, particularly around Alzheimer’s and Parkinson’s, go well beyond what the current evidence supports.
Universality. It does not work the same way for everyone. Baseline creatine levels, diet, age, and individual genetics all shape whether you respond, and how much.
Safety assumptions. What is low-risk for a healthy adult in their thirties requires very careful consideration for someone with kidney disease, certain metabolic conditions, or specific medications. The supplement industry’s one-size-fits-all framing is not just unhelpful in those cases. It is dangerous.
My position is straightforward. The science of creatine is genuinely interesting, and we need to understand it better. What I have no patience for is the layer of financial motivation and overclaims that ride the creatine science with hypes and misinformation. In most cases, this can be dangerous. This series exists to strip that away.
Where Nadia goes next, and where you might too
Nadia now understands the mechanism. She knows her low-meat diet likely puts her baseline on the lower end. She knows why her brain is as relevant a target as her muscles.
What she does not yet have is a protocol. Dose, timing, what to test before starting, realistic timeline, what to monitor. I will lay all of that out in the next article, the full evidence-based guide for a healthy adult with no diagnosis.
If you have an underlying condition, a family history of neurological disease, or are on medication, those situations have their own dedicated pieces later in this series.
The goal is not to tell you whether to take creatine. It is to give you enough of the actual picture to make that decision, with your doctor, from a position of real understanding.

Coming in this series
The healthy brain protocol.
Creatine and disease: which conditions connect and why? The Alzheimer’s and Parkinson’s data.
Creatine and the kidney: what the safety data actually shows.
The cancer angle. Contraindications and interactions.
And the precision medicine angle, why your individual biology changes everything.
If this was useful, share it with someone who has been asking the same questions Nadia was.
This article is everything. As someone who has been looking into getting into creatine from the fitness aspect, I too have thought “what exactly is creatine and why are all the fitness influencers telling me to take it?” Thus, I’ve always associated creatine with replenishing the body after intense workouts. Thanks for explaining the science behind creatine, it’s equally fascinating and important to understand the role it plays in our bodies!
First time I read about Creatine, I thought of an engine turbo charger. But the biological engineering doesn't make sense that way.
Later I was reading how fast glycolysis was compared to mitochondrial phosphorus oxidation... like 100 times faster. However if phosphorus creatine can take a ADP and quickly turn it back to ATP without a trip back to mitochondrial processing, that would speed the non-glycolysis ATP average cycle rate. And decrease the somewhat messy glycolysis pathway (and reduce lactate production). I suspect it also reduces mitochondrial reactive oxygen species "exhaust" which is useful in some ways but also dangerous. Also less heat since mitochondrial process is inefficient like any engine.
One puzzle is how phosphocreatine gets recharged after the ADP->ATP conversion. There has to be a rapid recycling process to avoid exhausting the process. What a hoot if the ATP utilization, which "consumes" a phosphate could be recycled into a phosphocreatine!!