
Not If. When.
How one woman refused to let the most terrifying disease you have never heard of write her ending, and what her story means for every one of us.

It started with a phone call on a birthday.
Sonia dialled her mother Kamni to wish her a happy 52nd. It was a call she had made every year, easy, ordinary, the kind of call you make on autopilot. But something was wrong. She could not name it yet. Her mother’s voice was there, but something behind it was not. Something essential was already beginning to go.
Within weeks, Kamni was in the hospital. Within months, she was on life support. By the end of that year, she was dead, and no one, not a single doctor, had been able to tell her family what had happened. The disease that took her did not have a name yet, not for them. There was no diagnosis. There was only the absence of a woman who had been there, and then was not.
The autopsy came later. And it changed everything.
• • •
The report named it: a rare genetic prion disease, a subtype known as Fatal Familial Insomnia. It was caused by a single mutation in Kamni’s DNA. One letter, in one gene, out of three billion. A typo so small you could not see it. A typo that had been enough.
And then came the sentence that reordered Sonia’s universe: the mutation was hereditary. Sonia had a 50/50 chance of carrying it herself.
She was 27 years old. She had just graduated from Harvard Law School. She had just gotten married. She had her whole life arranged in front of her like a table set for a long dinner, and now someone was telling her the table might be on fire.
“Suddenly, there’s this tear in the universe, and my mom is being sucked through it. No one can tell us what’s wrong, but something is really, really wrong, and it is snowballing, and it is everything. I’m looking into her eyes, and they are these black holes, and I am begging her to come back. But it’s like I’m shouting into the void.”
That is how Sonia Vallabh described watching her mother die. Not in a private journal. On the stage of the 2024 TED Conference, in front of thousands of people, with the steadiness of someone who has learned, through years of deliberate and agonising effort, how to hold grief and science in the same hands without dropping either.
Because by the time she spoke those words, Sonia was no longer just a grieving daughter. She was not practising law anymore. She had changed her career, and now she is a scientist. Her own scientist. Racing, with everything she had, to cure her own disease before it could take her the way it took her mother.
WHAT IS FATAL FAMILIAL INSOMNIA?
Before we go further into Sonia’s story, you need to understand what she is up against.
Fatal Familial Insomnia is not simply a sleep disorder. It is one of the most devastating and least understood diseases in all of medicine, and almost nobody outside of a handful of research labs has heard of it.
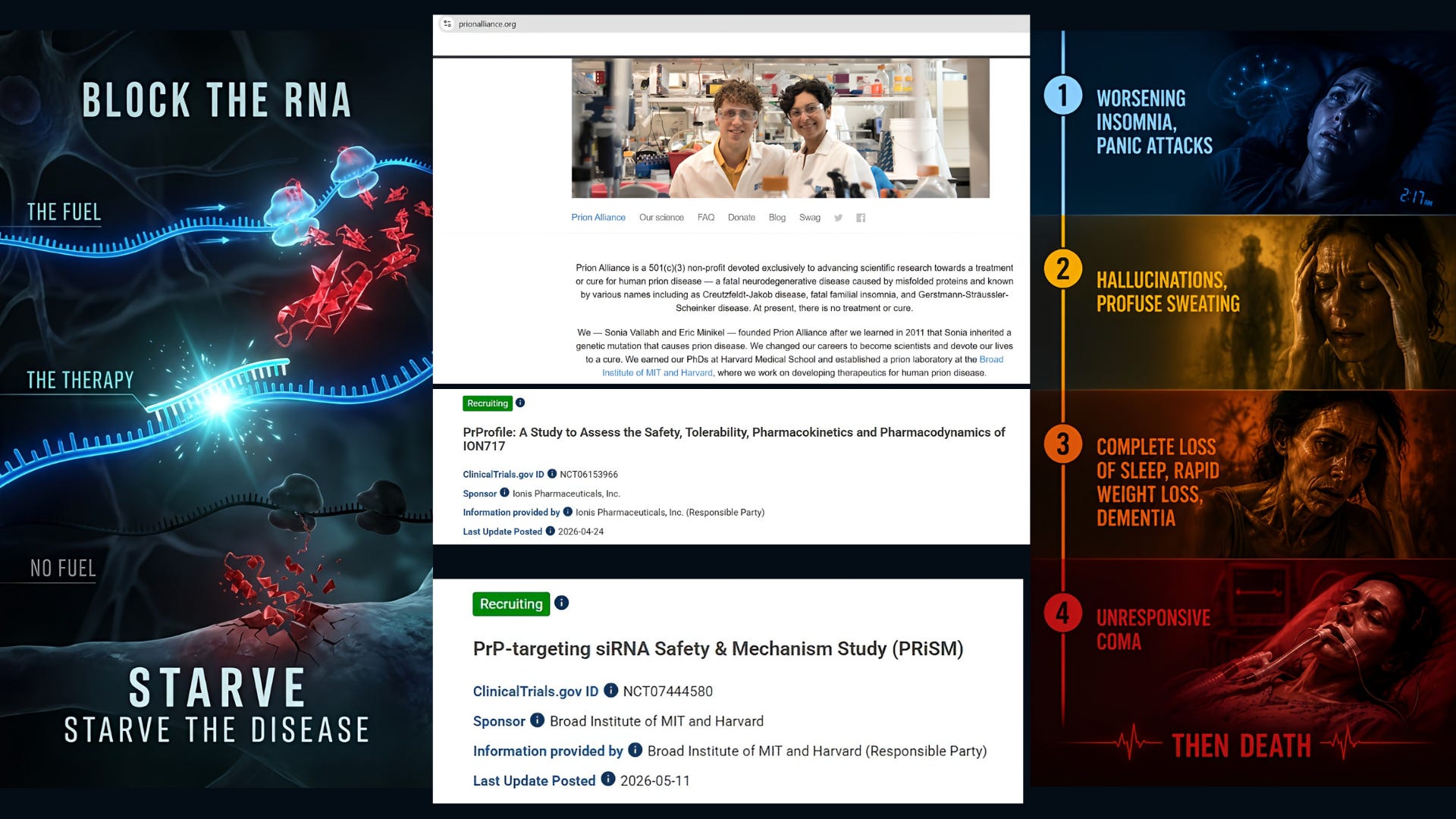
Let us start with the word “prion.” A prion is not a virus. It is not a bacterium. It is not something that enters your body from the outside. It is a protein. Specifically, it is one of your own proteins, called PrP, that has folded itself into the wrong shape. And once that misfolding begins, it triggers a cascade: the misfolded protein encounters normal PrP and converts it too, like a whisper spreading through a crowded room until everyone is saying the wrong thing.
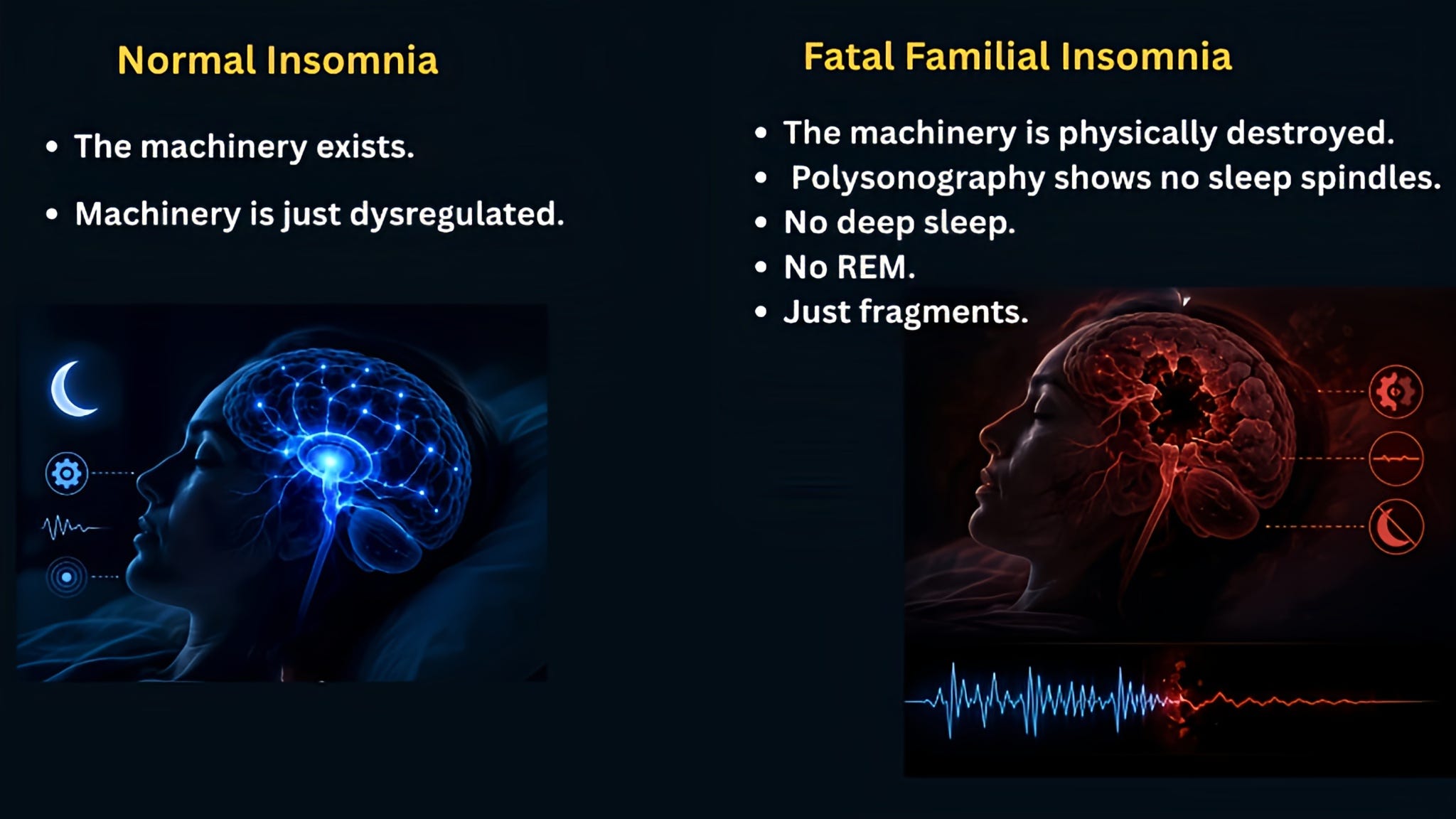
In Fatal Familial Insomnia, this process concentrates its damage in the thalamus, the small walnut-shaped structure deep in the centre of the brain that acts as the gatekeeper of consciousness. The thalamus governs the sleep-wake cycle. It regulates the autonomic nervous system. It filters sensory input and coordinates what reaches conscious awareness. When the thalamus begins to die, the results are catastrophic and unmistakable.
The clinical picture unfolds in stages. First comes the insomnia, not the ordinary sleeplessness of a stressful week, but a total inability to sleep, as though the switch has been permanently flipped to “awake.” The body cannot enter the deep restorative sleep cycles it needs to survive. Then come the autonomic disturbances: a racing heart, excessive sweating, fluctuating blood pressure, a body that no longer knows how to regulate itself. Then cognitive collapse. Hallucinations. Dementia. And finally, death. The average course from first symptom to the end is eighteen months.
There is no treatment. There is no cure. And because the disease is genetic, the tragedy does not end with one person. It moves through families, generation after generation, carried in a single letter of DNA.
Worldwide, only a few dozen families are known to carry this specific mutation. In the entire history of medical literature, fewer than 200 cases have ever been documented. It is, by almost any measure, one of the rarest diseases on earth.
And yet the lessons it holds for all of us are enormous.
A LAWYER BECOMES A SCIENTIST
Sonia and her husband Eric Minikel did something that almost no one does when confronted with a terminal genetic diagnosis. They did not grieve quietly and wait. They did not turn to unproven remedies. They did not hand their fate to someone else and hope.
They built a laboratory.
Within weeks of Sonia’s positive test result, both of them quit their careers, Sonia from law, Eric from transportation engineering. They took entry-level positions at research labs, doing work far beneath their education, pipetting samples and washing equipment alongside students half their age. They enrolled in night classes. They read scientific papers that they did not yet have the vocabulary to understand. They cold-called researchers around the world, introducing themselves simply as a family affected by prion disease who wanted to help.
Some scientists called them back. Most did not. They kept calling.
By 2014, both Sonia and Eric had enrolled in PhD programs in Biological and Biomedical Sciences at Harvard. They graduated together. They founded the Prion Alliance, a nonprofit dedicated to funding and accelerating therapeutic research. They now lead Prions@Broad, a research group at the Broad Institute of MIT and Harvard, working at the very edge of what science currently knows how to do.
Sonia has written about this transformation in the New England Journal of Medicine, one of the most prestigious medical journals in the world, describing the concept of the “patient-scientist.” The idea is straightforward: when you are both the researcher and the patient, when your own survival depends on the outcome of the experiment, you bring a quality of urgency and attention that no external motivation can replicate.
She describes their approach with a metaphor that has stayed with me since I first read it. “Driving at night in the fog. You can only see as far as your headlights, but you can make the whole trip that way.”
You do not need to see the end. You only need to see what is directly in front of you and keep moving.
THE WELLNESS EPIDEMIC
Here is where I need to speak to you directly, as someone who has spent years studying disease and trying to translate science for the people who need it most.
When a diagnosis is terrifying, when medicine says “we don’t know” or “we can’t cure this yet,” a space opens up. And into that space rush all manner of things. Some are well-meaning and simply misguided. Some are cynical and extraordinarily dangerous. All of them understand one thing very clearly:
Fear is the most monetisable emotion in the world.
Belle Gibson built one of Australia’s most successful wellness brands on the claim that she had healed her own brain cancer through diet and alternative therapies. She had not. There was no cancer. The diagnosis was fabricated. But tens of thousands of people trusted her, bought her cookbook, followed her protocols, and in some cases, genuinely diverted from medical treatment toward her methods. When the truth emerged, the damage had already been done.
Steve Jobs was diagnosed in 2003 with a pancreatic neuroendocrine tumour, one of the slowest-growing and most treatable forms of pancreatic cancer. His surgeon told him it was operable. His prognosis, had he acted immediately, was genuinely good. He did not act immediately. For nine months, he pursued dietary interventions, acupuncture, herbal remedies, and the counsel of a psychic. By the time he agreed to surgery, the cancer had spread. His own biographer described this delay as one of the few decisions in his life he genuinely regretted. He died in 2011.
I am not sharing these stories to judge anyone. Fear does extraordinary things to human reasoning. The desire to feel in control of something terrifying is not weakness; it is one of the most human responses imaginable. The juice cleanse, the supplement, the testimonial from someone who swears they healed themselves, these things feel like agency when medicine offers uncertainty. I understand the appeal completely.
But an agency built on false information is not an agency. It is the illusion of it. And the difference between the two can cost you your life.
This is exactly why I write about disease the way I do. Not to replace your doctor. Not to frighten you into paralysis. But to hand you the one thing that no influencer can sell and no algorithm can manufacture: the actual facts. The peer-reviewed, tested, challenged, sometimes revised, sometimes inconvenient facts. Because when you understand what a disease actually is, how it works at a cellular and molecular level, what the evidence for various treatments actually shows, you become someone who is very difficult to deceive.
You become your own best advocate. And that is the most powerful thing you can be.
WHERE THE SCIENCE STANDS
Back to Sonia. Because the science she and her team are building deserves your full attention.
The central logic of their therapeutic approach is elegant and compelling. Prion disease requires the prion protein. If you reduce the amount of PrP the brain produces, you reduce the fuel available for the disease to propagate. You do not chase the misfolded protein once it has spread. You reduce the supply before the cascade can begin.
In animal models, this strategy has shown remarkable results. Reducing PrP extended survival. In some experiments, it reversed symptoms that had already appeared. The science, while still evolving, pointed clearly in one direction.
In 2023, that direction became a clinical trial.
ION717 is an antisense oligonucleotide, a carefully designed molecule that silences the gene responsible for producing PrP. It is administered by lumbar puncture, directly into the cerebrospinal fluid that bathes the brain and spinal cord. In December 2023, the PrProfile Phase 1/2a trial opened enrollment. By December 2024, all 56 participants had been enrolled across sites globally. Preliminary data showed an encouraging safety and tolerability profile, and as of early 2026, the trial has reopened to test a higher dose level in the hope of achieving even deeper PrP reduction.
This is the first time in history that a drug designed to lower the protein that causes prion disease has been tested in living human beings.
Separately, Sonia’s own lab published work in 2024 demonstrating that a gene-editing approach could silence the prion gene by up to 90 % in mouse models. A 2025 study showed that altering the PrP-producing gene extended mouse lifespans by 52 %. In Italy, a long-running trial has been testing doxycycline as a preventive treatment in at-risk family members who carry the mutation but have not yet developed symptoms.
None of this is a cure. Not yet. But the trajectory is unlike anything this field has seen before.
NOT IF. WHEN.
Sonia Vallabh is now in her late thirties. She carries the mutation that killed her mother. She knows what that means clinically. She also knows, better than almost anyone alive, exactly what is being done about it and how close that work might be to mattering.
I think about what it takes to hold both of those things at once. The knowledge of what is coming and the absolute refusal to be passive in the face of it. The grief that never fully leaves and the daily discipline of transforming it into data, into experiments, into results.
She is not waiting to be saved. She is building the thing that might save her. And in doing so, she is building something that could save others who carry this mutation, and potentially lay the groundwork for treatments across the entire spectrum of prion diseases.
This is what I want you to take away from her story, and from this piece.
Not everyone can become a scientist. Not everyone can enrol in a PhD program, found a nonprofit, or run experiments at one of the world’s premier research institutions. That is not the point. The point is the posture. The refusal to hand your health entirely to someone else and hope for the best. The commitment to learning the real facts, even when they are frightening, even when they are uncertain, even when they do not come with the reassuring simplicity of a wellness influencer telling you that one simple change will fix everything.
Ask questions. Read widely. Get a second opinion. When a claim sounds miraculous, ask who funded the study. When a testimonial goes viral, ask what it is selling. When your doctor dismisses a symptom you know is real, push back. When the science is genuinely uncertain, sit with that uncertainty rather than filling it with something comfortable but false.
Your health belongs to you. Not to a brand. Not to an algorithm. Not to a doctor who has seven minutes and a waiting room full of patients. To you.
Sonia Vallabh looked at a death sentence written in her own DNA and said: not if. When.
You can say the same thing about your own health, in whatever form the fight takes. Not passively. Not with false hope. But with real knowledge, real questions, and the stubborn, beautiful refusal to stop fighting.
If you found this piece valuable, please share it with someone who needs it. All clinical trial information referenced here is publicly available through ClinicalTrials.gov. For more on Sonia Vallabh’s work, visit the Prion Alliance at prionalliance.org.
Really great article, and I like that you kept bringing it back to the bigger picture for people who have to navigate a murky medical and ‘wellness’ system.